Achilles Tendon Pain
In Greek mythology, the Achilles’ heel is avowed to be a point of weakness, especially in someone who is otherwise very fit. Indeed, it might take the actions of a vigorous greek warrior to injure the strongest tendon in the body. Incapacitating the Achilles tendon requires a great deal of tensile load over time – or in just a very unfortunate instant.
If a basketball player jumps into a crowd fighting for the rebound and comes down on someone else’s foot, that can create enough acute stress to the Achilles tendon to partially or completely rupture the tendon away from its attachment to the back of the heel. Season over. Surgery to reattach a ruptured tendon to the calcaneus bone is fairly urgent to sustain the athletic life of the gastrocnemius and soleus muscles and the portion of the tibial nerve for those muscles. Highly motivated recovery in physical therapy takes 6 months, but up to 12 months isn’t uncommon.
Why do I have Achilles pain even though I’m not a greek warrior with a 48’ vertical jump like Michael Jordon?
Soleus Trigger Points
The gastrocnemius has two muscle sections on the outer layer of the calf and can be very pronounced in cyclists and body builders. Stretchy muscle fibers transform to the dense Achilles tendon mid calf and is made of inelastic connective tissue, mostly collagen. The powerful tendon carries the tensile load of the muscle action to create movement at the bone.
The muscle to tendon connection point is vulnerable to small tears due to the change in fiber type. Tennis players and participants of other harsh cutting sports can experience micro tears in the medial gastrocnemius at the musculotendinous junction, and scar tissue from multiple small strains can build over time.
The soleus muscle belly is directly under the transition of the gastrocnemius muscle to tendon. 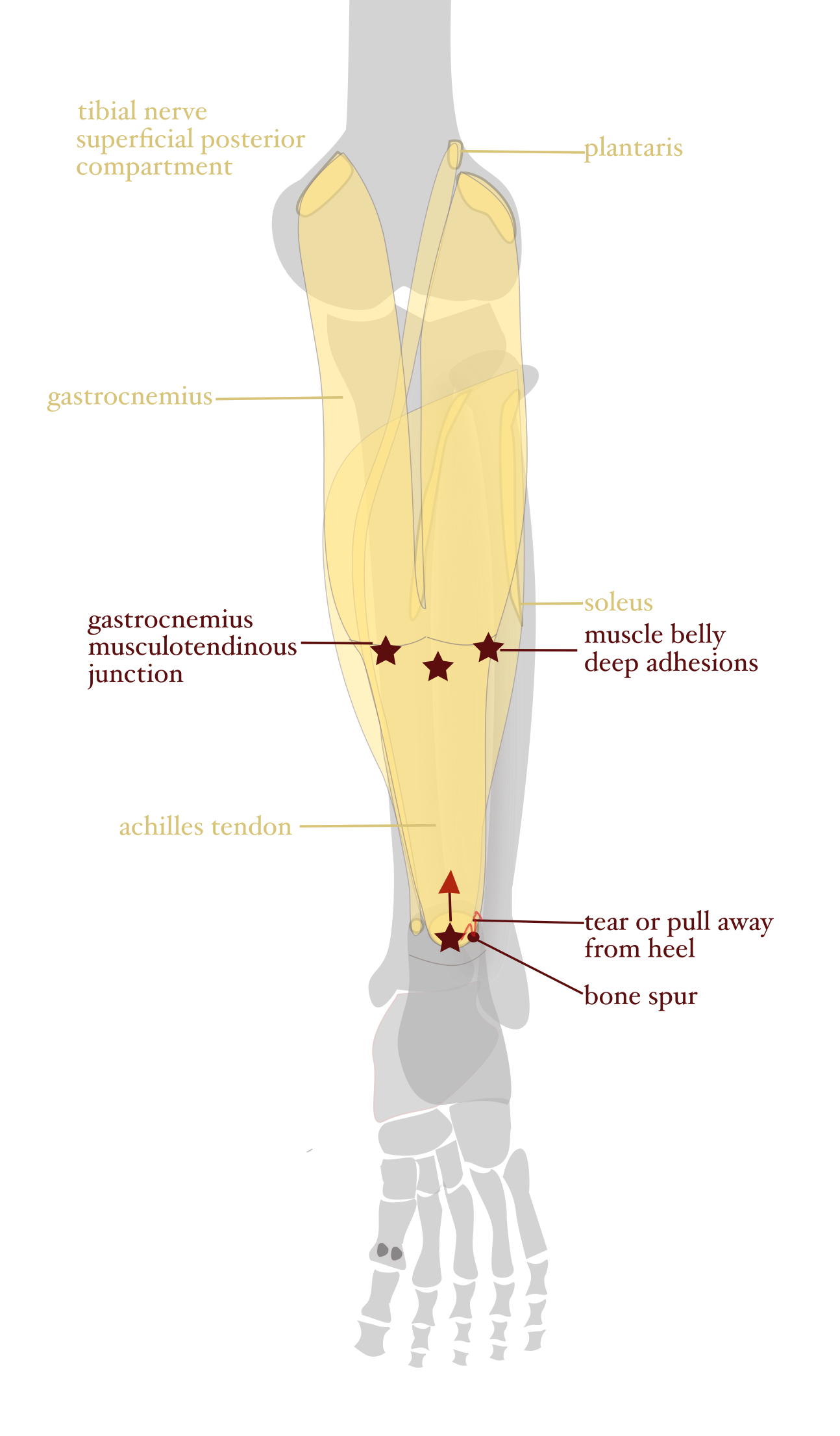 Trigger points often develop in the belly of a muscle. Getting to the deep adhesions in the soleus muscle under the stronger superficial muscle can be challenging. The soleus is wider than the gastrocnemius, so approaching the soleus at the side of the calf can be very productive. Myofacial release with a ball or stick can warm up the soleus making it easier to get under the gastrocnemius.
Trigger points often develop in the belly of a muscle. Getting to the deep adhesions in the soleus muscle under the stronger superficial muscle can be challenging. The soleus is wider than the gastrocnemius, so approaching the soleus at the side of the calf can be very productive. Myofacial release with a ball or stick can warm up the soleus making it easier to get under the gastrocnemius.
The achilles tendon is like string cheese in that the superficial gastrocnemius forms the most superficial fibers of the tendon, and the soleus forms the deep fibers. Both muscle tendons generally do the same job, but since the soleus tendon does not cross the knee joint, it has different behaviors in certain movements. For example, a ski jumper with completely straight legs will more likely injure the deep soleus in a rough landing. The gastrocnemius muscle crosses the knee joint and can absorb the shock better. In this case, the superficial Achilles tendon fibers are normal, but the deep soleus fibers closer to the bone are very tight.
When a small portion of the tendon pulls away from the heel, a gap is created between the tendon and the bone. Calcium from the bone patches the gap. A bone spur can form, especially from ill fitting shoes or a dramatic change in the heel type of the shoe. Sometimes, it’s necessary to remove the spur, but myofacial release of the muscles and tendon creating the pulling force can be productive.
Deep Posterior Compartment Muscles
Shin guards in soccer prevent vulnerable beginners from getting kicked in the legs as every little one on the field is chasing after the ball in a pack. More experienced players with cleats or spikes will engage in an attack to attempt to steal the ball, and may, on occasion, inadvertently kick a defender’s leg rather than the ball.
Cross country ski binding accidents especially with short boots, martial arts kicks to the opponent’s leg, a foot stuck in a the stirrup of a horse’s saddle are just a few of the types of injuries that can cause damage to muscles of the deep posterior compartment muscles. 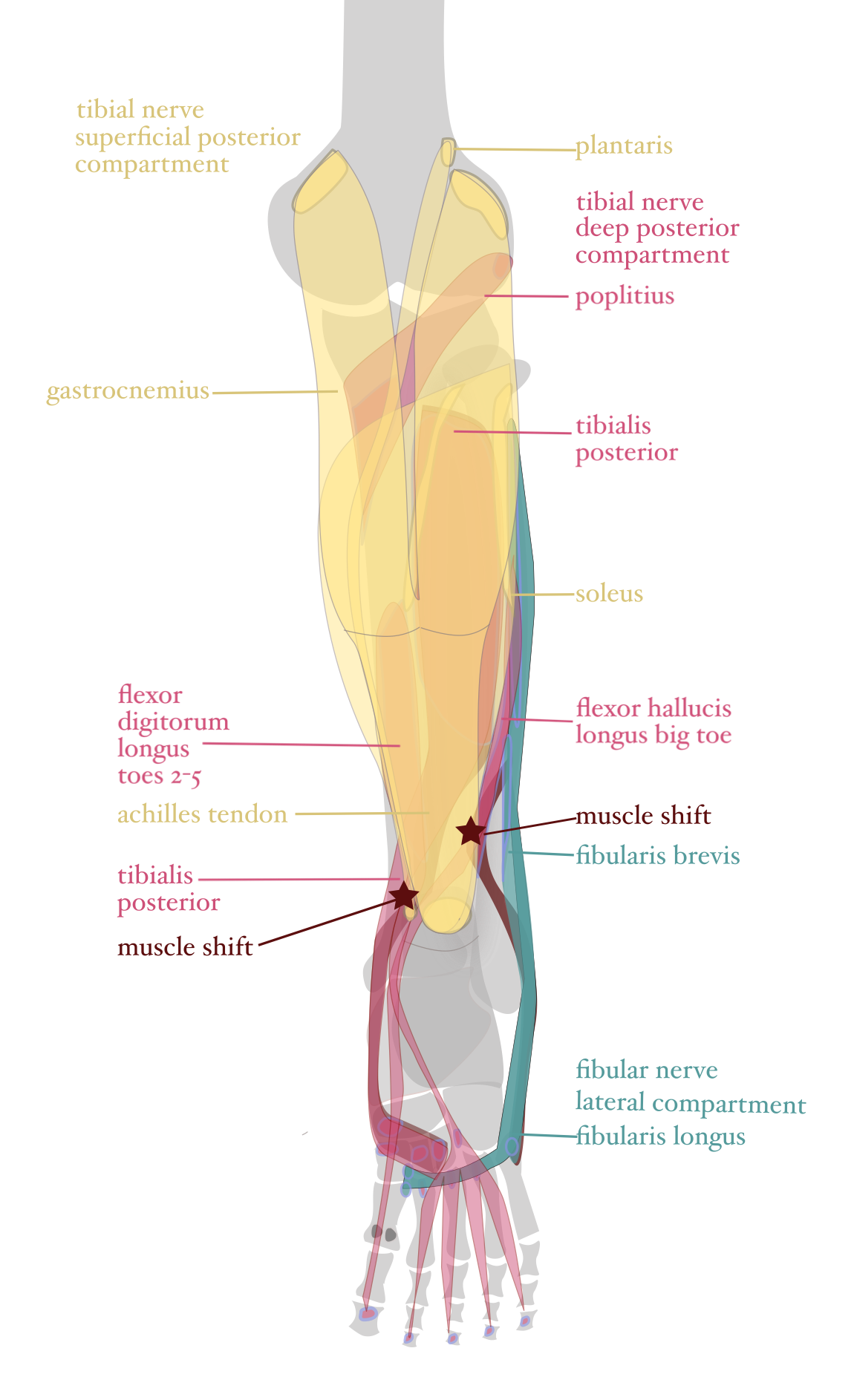 This external force can shift muscles directly into the Achilles tendon creating adhesions in the displaced muscle. Ankle strains can also shift deep posterior compartment muscles that cross the ankle joint into the tendon itself or at its attachment to the heel.
This external force can shift muscles directly into the Achilles tendon creating adhesions in the displaced muscle. Ankle strains can also shift deep posterior compartment muscles that cross the ankle joint into the tendon itself or at its attachment to the heel.
The deep compartment muscles can be hard to reach under the gastrocnemius and soleus, but can be worked from either side of the leg similar to the soleus strategy.
One effective way to evaluate muscle position is to place your hand on the target muscle and then perform the motion of the specific group of muscles. For example, the lateral compartment muscles evert or rotate the foot outward. The deep posterior compartment muscles invert or rotate the foot inward. Both superior and deep compartment muscles plantar flex or point the foot downward. If you touch the area behind the inside ankle bone and then rotate the foot inward from the big toe, you can feel the movement of the deep posterior muscles. Now move your hand a bit to press the area just inside the heel and then point the foot downward to test the motion of the gastrocnemius and soleus through the Achilles tendon. Alternate between inversion of the foot and plantar flexion to see if you can feel distinct muscle contractions. If the tibialis posterior has an adhesion to the Achilles tendon or heel, you might feel a tug that resists the action of moving the foot inward. Muscle palpation takes a lot of practice, but can be very helpful to see if the muscle contraction follows its designated line of movement. Studying muscle attachment sites and actions can help learn to follow a muscle line to see if there are any detours that can contribute to chronic pain.
Pro Tip: Pressing or pinning a muscle at an adhesion or trigger point, then stretching the muscle, aka pin and stretch, can loosen the scar tissue and correct changes in muscle or tendon fiber direction. For example, pin the tibialis posterior muscle behind the medial ankle bone, then evert the foot outward. The opposing muscle action, eversion, of the fibularis muscles will stretch the tibialis posterior.
Greek mythology may have gotten it right about finding the weakness of a warrior in the Achilles tendon, but I profess that weekend warriors should be included in those epic adventures.
![]() Author: Mary Bai of Tibialis, LLC is practicing Clinical, Orthopedic, Medical Massage in Redwood City, CA.
Author: Mary Bai of Tibialis, LLC is practicing Clinical, Orthopedic, Medical Massage in Redwood City, CA.
Contact: mary@tibialis.com